
![]()
Evidence-based Interventions to Prevent Childhood Undernutrition in Pakistan’s Punjab




Background
Pakistan’s Punjab province has access to rich district-representative household survey data from the Multiple Indicators Cluster Survey (MICS). Five survey rounds were conducted in 2004, 2007, 2011, 2014, and 2018. However, a lack of secondary analysis of these data in the thematic area of childhood undernutrition has obstructed policymakers from undertaking evidence-based policy decisions. Based on MICS Punjab data and empirical analysis, this policy note identifies evidence-based interventions and entry points that can help policymakers realign existing policies to reduce childhood malnutrition.
A trend analysis was conducted on data from previous survey rounds to provide insights into gray areas where current policies have remained ineffective in controlling undernutrition. Interesting evidence was obtained from raw data of 38,495 under-five children acquired from the Punjab MICS 2018. These data were also used to identify high-risk factors associated with childhood undernutrition using multivariate logistic regressions. To allow for the impact to vary by age group, the analysis was also conducted on two subsamples disaggregated by age groups of 6 – 35 months and <6 months. The adjusted risk of the independent variables was determined by calculating the odds ratios (OR) with 95% confidence intervals.
Prevalence and trends
Every third child under the age of five years is stunted (31.5%) in Punjab, and most of them live in the 11 districts of South Punjab. The stunting rates declined by 10 percentage points, from 42% in 2007 to 31.5% in 2018, typically declining at a faster pace in Central-North than in South Punjab. Moreover, a district-level trend analysis suggests that the prevalence of stunting has increased, rather than decreased, in more than two dozen districts, viz., Rahim Yar Khan, Lodhran, Rawalpindi, Attock, Chakwal, Jhelum, Bhakkar, Khanewal, Multan, Faisalabad, Chiniot, Bahawalpur, and Bahawalnagar. Thus, there is a strong possibility that the intervention strategies have not been equally successful in all districts.
Every 1 in 5 children in Punjab is underweight (21.2%). Interestingly, the prevalence of underweight children remained stable between 2007 and 2014, but fell dramatically in the later period, from 34% in 2014 to 21.2% in 2018. Further improvements are required if this trend continues. A regional comparison revealed that the prevalence of underweight children was significantly higher in South Punjab (26.4%) than in other Punjab (18.7%). The highest incidence in South Punjab was found in Rajanpur (34%), Rahim Yar Khan (33%), and D.G.. Khan (32%) districts.
In terms of the prevalence of wasting, every 1 in 13 children in Punjab is wasted (7.3 %). Initially, the wasting rate increased from 14.3% in 2007 to 16.2% in 2014; however, during the next four years, the wasting rate decreased from 17% in 2014 to less than 8% in 2018. If this trend continues, we can expect further improvements over the next decade.
These results suggest that the intervention strategies implemented in the post-2007 period were largely responsible for the observed decrease in stunting, underweight, and wasting rates. Since the population growth in the province still stands at 2.6%, the prevalence of high stunting, underweight, and wasting rates translates into an increase in the absolute number of undernourished children. Therefore, evidence-based strategies are required to promote investment in nutrition-specific programs, particularly in lagging districts.
Strong, healthy mothers make for strong, healthy children
Our analysis was based on microdata of 38,495 children aged 0 – 59 months, 18,688 children aged 6 – 35 months, and 4,453 children aged 0 – 5 months, and showed that the prevalence of stunting and underweight was more common in older children, but the prevalence of wasting was much more common in younger children. Moreover, the undernutrition rates were higher in boys than in girls.
Figure 1 shows that the stunting rate among low-birth-weight children was 34%, compared to 26% for average-sized children. Similarly, underweight and wasting rates were higher in low-birth-weight children than in the average. A birth spacing of less than 24 months increased undernutrition, as such children had relatively higher stunting, underweight, and wasting rates than children with higher birth intervals. Additionally, stunting and underweight rates were relatively higher among children born to mothers aged < 20 years than among all others.
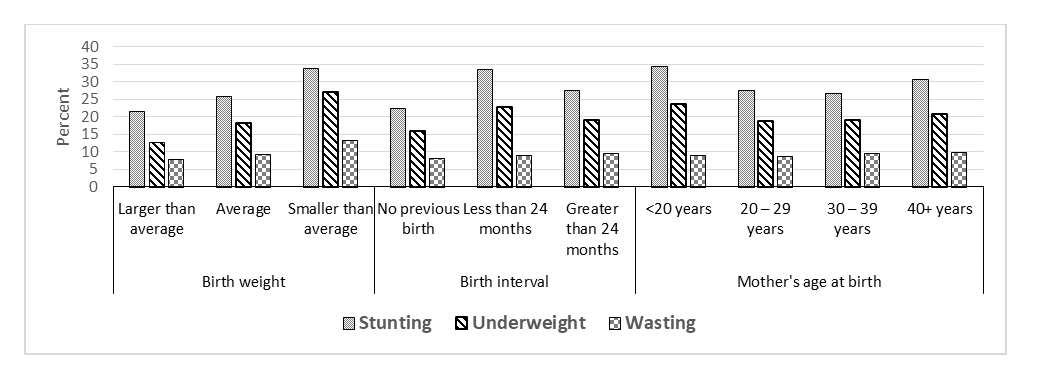
Figure 1: Undernutrition by birth weight, birth interval and mother’s age
Source: MICS Punjab
Lack of maternal education has a significant impact on the prevalence of childhood undernutrition. Approximately 44% of mothers in the sample had no education, 30% had below secondary education, and only 26% had secondary education or better. Figure 2 clearly indicates that no maternal education or low maternal education raises the chances of childhood undernutrition, whereas the incidence of stunting, underweight, and wasting declines as the mother’s education increases. Furthermore, childhood undernutrition is negatively associated with household wealth status, as measured by the wealth quintiles (Fig. 2). Stunting, underweight, and wasting rates were highest for children from the poorest wealth quintiles and lowest for children from the richest wealth quintiles.
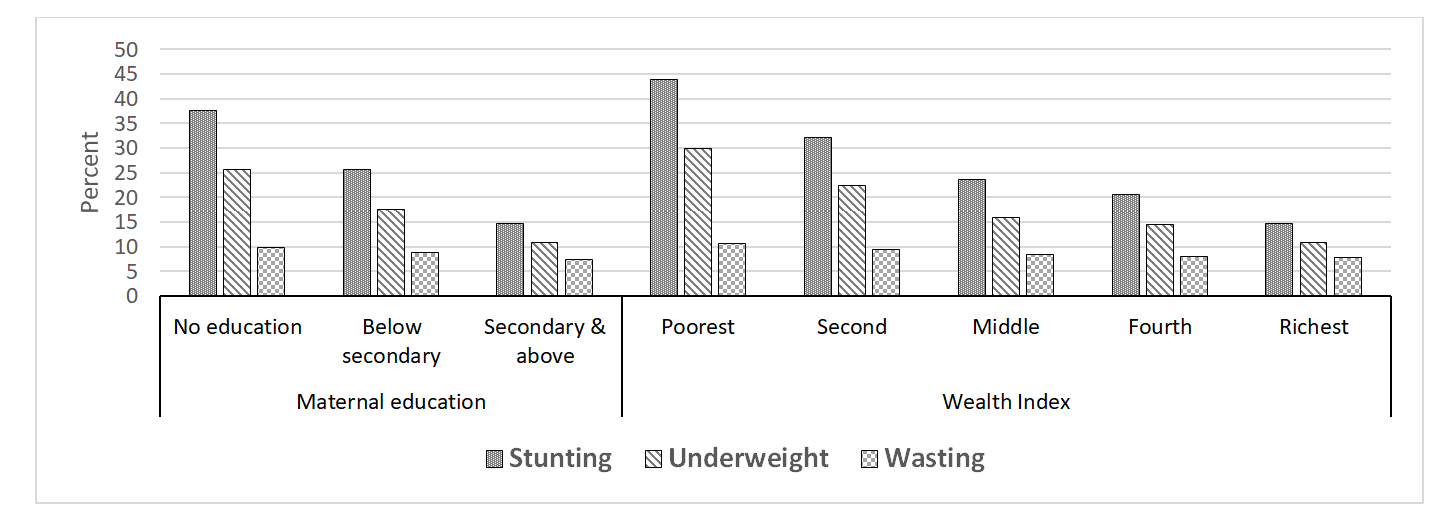
Figure 2: Undernutrition by maternal education and wealth quintiles
Source: MICS Punjab
Among children aged 0 – 5 months, the prevalence of undernutrition was higher in cases where the mothers had received no antenatal care. About 26% of children aged 0 – 5 months were not delivered in a hospital, and the undernutrition of such children was marginally higher than that of children who were delivered in a hospital. Approximately 9% of the mothers had unassisted delivery, and their children were found to have higher stunting, underweight, and wasting rates than those who had assisted delivery.
One in every four pregnant mothers did not receive tetanus shots during pregnancy. For these mothers, the prevalence of stunting, underweight, and wasting in children was three-, four-, and two percentage points, respectively, higher than for those who received tetanus shots. It is well known that exclusive breastfeeding in children aged 0 – 5 years provides natural protection from diseases, infections, and diarrhea. Those who were not exclusively breastfed had significantly higher stunting, underweight, and wasting rates than those who were exclusively breastfed. A small proportion of children (11.4%) who consumed infant formula had higher rates of stunting, underweight, and wasting than those who did not take infant formula.
Of the 18,688 children aged 6 – 35 months, 11, 867 (64%) did not consume a balanced diet, eating less than four food groups out of seven recommended by the WHO. Stunting, underweight, and wasting rates were respectively four-, five-, and one-percentage point higher, respectively, in children who had no minimum dietary diversity than in children in the base category. The prevalence of stunting, underweight, and wasting was also significantly higher among children who were not completely vaccinated, had diarrhea in the last two weeks, and had fever in the last two weeks, compared with children in the base categories.
How can childhood undernutrition be prevented?
Poverty and lack of maternal education are the two leading causes of childhood undernutrition. The association between household wealth and childhood undernutrition is well-known and was confirmed by our results. It seems very likely that due to binding income constraints, these households were unable to invest in the health of the mothers and children, leading to long-term and short-term nutritional deficiencies and, ergo, warranting targeted interventions.
Lack of maternal education has emerged as another key risk factor, perhaps because uneducated mothers do not better utilize healthcare facilities, including prenatal and postnatal care, maintain an understanding of disease management, or value the importance of exclusive breastfeeding and dietary diversity for children aged 6 – 35 months. Low birth weight is a problem associated with maternal education because a lack of maternal care activities before and during pregnancy leads to undernutrition. Therefore, policies that incentivize the uptake of selected health and nutrition services by pregnant and lactating women with children below the age of two years should be adopted.
Short birth intervals have unfavorable outcomes for child nutrition, highlighting the importance of lengthening the birth spacing. Suitable measures are required to encourage women to increase their birth spacing. Policies that promote effective campaigns for counselling women to extend exclusive breastfeeding, including the use of family planning services and the increased availability of socio-culturally and legally compliant abortion services, can help lengthen birth spacing.
Early marriages are a common issue in Pakistan. Children born to teenage mothers had significantly higher odds of being stunted and underweight. Although delayed marriages are desirable because of their positive impact on the state of undernutrition, this is a hugely controversial issue because marriage laws are vague and do not provide clear instructions on the minimum age for girls to contract marriage. The Government of the Punjab, through its elected assembly, may want to amend the law for girls’ minimum marriage age by officially defining anyone less than 18 years of age as a child.
Access to information has emerged as another leading correlate of malnutrition. Households with a lack of access to mobile phones and the internet were observed to have significantly higher odds of childhood undernutrition. This finding has important policy implications for providing affordable internet and mobile phone services to reduce the burden of childhood undernutrition, especially in districts where the burden is relatively high.
Unsurprisingly, the occurrence of diarrhea and fever is also directly linked to childhood undernutrition because infections and diarrhea both reduce appetite and interfere with the digestive system and food absorption.
Nearly 14% of the sampled children lived in households that practiced open defecation rather than using a latrine. These children are more likely to be shorter, suggesting a link between open defecation and disease prevalence. Eliminating open defecation by 2030 is part of the sanitation target of the Sustainable Development Goals (SDGs), and a clear understanding is required of the target needed to achieve this goal.
Complementary feeding in children aged 6 – 35 months is an important correlate of childhood undernutrition. Strategies that promote counseling to improve complementary feeding could significantly reduce malnutrition.
Lack of exclusive breastfeeding is a leading cause of undernutrition in children below six months. Interventions should provide mothers with basic education on adequate nutrition using the available health services in the province. Strategically positioned 24/7 governmental centers and hotlines can play a vital role, providing both safe delivery services as well as appropriate advice on postnatal care.
This post is based on Burki, Abid A. (2022). Relative Importance of the Risk Factors of Stunting, Underweight and Wasting in Under-Five Children in Pakistan’s Punjab: Evidence from MICS data. A Report Commissioned by Punjab Bureau of Statistics, Government of Punjab, in collaboration with UNICEF, Pakistan.
Abid Aman Burki, Adjunct Professor (Economics), LUMS

Abid Aman Burki
Mahbub ul Haq Research Centre at LUMS




Postal Address
LUMS
Sector U, DHA
Lahore Cantt, 54792, Pakistan
Office Hours
Mon. to Fri., 8:30 a.m. to 5:00 p.m.